
Facial feminisation surgery, known as FFS (Facial Feminization Surgery), is one of the gender affirmation procedures that generates the most questions before the first consultation. And no wonder: unlike other surgeries, FFS is not a single procedure but a customised combination of interventions on different areas of the face. Knowing which ones you need, in what order it makes sense to do them and what real impact each one will have on your appearance are questions that no one can answer without studying your specific anatomy, but understanding the logic behind the planning helps you arrive at the consultation with much clearer ideas.
This article is not intended to replace that individualised assessment, but to explain how the FFS planning process works, which areas of the face have the greatest perceptual impact in terms of feminisation, and what factors determine whether it makes sense to do it all in one session or spread it over several stages. Useful information whether you are just starting to find out, or if you have a consultation coming up and want to go in with well-formulated questions.
What exactly is FFS and how does it differ from conventional cosmetic surgery?
Facial feminisation surgery is not cosmetic surgery in the conventional sense of the term. While a rhinoplasty aesthetics or a facelift seek to enhance or rejuvenate a person's appearance without altering their gender perception, the FFS has a different objective: to modify facial structures whose morphology is socially perceived as masculine in order to achieve a more feminine appearance consistent with each patient's identity.
This means working with bony structures, not only with soft tissues. The forehead, supraorbital arch, jaw, chin or nose have different morphological characteristics depending on biological sex. Hormone therapy with oestrogen may soften some soft tissue features over time, but it does not change the underlying bone structure. This is where FFS has a definitive effect.
This is an important nuance: FFS is gender-affirming reconstructive surgery, not just cosmetic. That approach changes how it is planned, how outcomes are evaluated, and what degree of transformation is possible and reasonable to expect.
The three zones of the face and their role in gender perception
When a FFS surgeon analyses a face, he or she does so by dividing the facial space into three thirds: upper, middle and lower. Each has different characteristics and a different weight in how the brain processes gender indicators in a face.
Upper third: the forehead and hairline
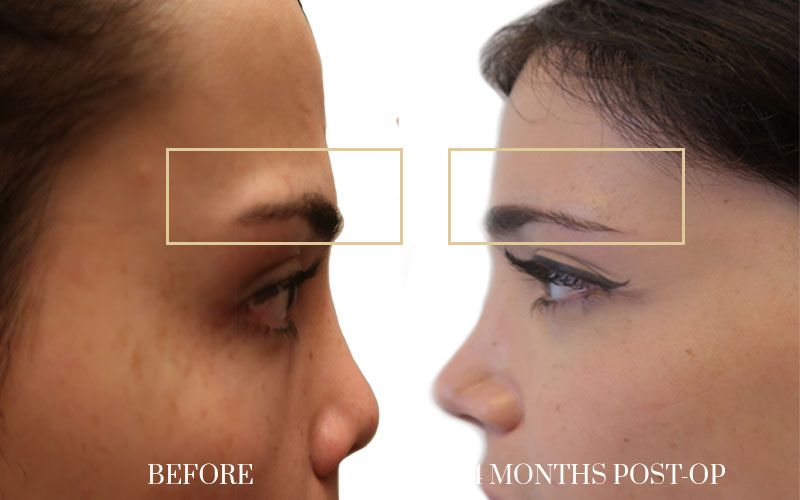
The forehead is, according to most studies on facial perception, the area with the greatest impact on the gender reading of a face. Male foreheads tend to have a protrusion of the supraorbital bone (the ridge just above the eyebrows), a more backward sloping forehead and a more receding hairline. Female foreheads are generally more vertical, more rounded and with a smooth transition from the bone to the scalp.
Feminisation of the forehead may include filing or reshaping the supraorbital arch, raising the eyebrows to achieve a more open expression, and in some cases lowering the hairline to reduce the proportion of the forehead. It is one of the procedures with the greatest impact on the overall result and, at the same time, one of those that requires the most technical expertise, because it involves working on bone in an area close to important structures.
Middle third: nose, cheekbones and lips
The middle third of the face concentrates several procedures that, combined, have a very relevant synergistic effect. The nose is one of the most requested areas: a feminising rhinoplasty does not simply seek to reduce the size of the nose, but to adjust its proportions and angles so that it fits harmoniously with the rest of the features. This may include softening the bridge of the nose, refining the tip or adjusting the nasolabial angle.
The cheekbones also play an important role: adequate volume in the malar area helps to create a more feminine facial oval. Depending on the case, this can be addressed with hyaluronic acid or autologous fat fillers, or with malar implants if a more permanent and defined projection is sought. The lips, on the other hand, respond very well to non-surgical techniques such as the lip lift, which shortens the distance between the nose and the upper lip and gives a more youthful and feminine appearance without the need to use volumisers continuously.
Lower third: jaw and chin
The lower third of the face is the most common area of the face that reveals a male bone structure. Jaws with sharp angles and a square or prominent chin are features that FFS can significantly transform by reducing jaw angles and mentoplasty, which modifies the shape of the chin to make it narrower, rounder or slimmer depending on the morphology of each patient.
The effect of these changes in the lower third is particularly noticeable in frontal views and photographs, as it defines the facial oval towards a shape more characteristic of female morphology.
A single surgery or several stages? How is this decision made?
One of the most frequently asked questions in pre-FFS consultations is whether all the procedures can be done at the same time or whether they need to be spread out over time. The answer depends on a number of factors that the surgeon must assess on an individual basis, but there is a general logic to understand.
Advantages of doing several procedures in one session

Combining procedures in a single procedure has clear advantages: the total number of general anaesthetics is reduced, the overall recovery time is shorter than if several surgeries are performed separately, and the final result can be planned more coherently because the surgeon works with an overall view of the face from the outset. For many patients, doing FFS in a single session is the most medically and logistically efficient option.
In general, upper, mid and lower face procedures can be combined without problems if the patient's general health is good and surgical time is kept within safe limits. Dr. Richard Fakin plans each case individually to maximise the outcome while minimising risk, and assesses at each consultation which combinations make sense for each particular anatomy.
When does it make sense to spread it over several stages?
In other cases, spreading the FFS over two or more phases may be the most appropriate option. This is the case when the number of procedures required is very high and combining them all in one session would lengthen the surgical time excessively, when the patient prefers to observe the outcome of a first phase before making decisions about the next one, or when medical considerations dictate shorter interventions.
The phased approach also allows planning to be adjusted throughout the process: after seeing how the outcome of the first surgery evolves and how the tissues adapt, the surgeon and patient can make more informed decisions about which additional procedures make sense and which are no longer necessary.
Which procedures have the most impact on the overall outcome
Not all FFS procedures have the same weight on the perceived outcome. From a gender perception point of view, there are interventions that generate more striking change and others that refine important details but whose impact is more subtle. Understanding this hierarchy helps to prioritise when there are constraints of time, budget or personal preference.
Feminisation of the forehead and reshaping of the supraorbital arch are generally considered to be the procedures with the greatest impact on the gender reading of the face. The forehead is the first area that the brain processes when analysing a face, and softening this area has an effect that is perceived globally even if the observer cannot identify exactly what has changed.
Jaw reduction and mentoplasty also have a very significant impact, especially on the silhouette of the face when viewed from the front. They transform the facial oval from an angular, square shape to a narrower, rounder shape in the lower third, which is a very clear marker of facial femininity.
Feminising rhinoplasty and middle third procedures have a more subtle but equally important effect on overall harmony. When combined with upper and lower third procedures, the result is much more than the sum of its parts: each area reinforces and balances the effect of the others.
The role of hormone therapy in FFS planning
Estrogen hormone therapy produces changes in the soft tissues of the face that are relevant to FFS planning. Over time, it can redistribute facial fat, soften skin texture and slightly reduce some angular features. These changes do not affect bone structure, but they can influence the decision as to which soft tissue procedures are necessary and to what extent.
For this reason, many medical teams recommend waiting at least one year of stable hormone treatment before planning FFS, in order to evaluate the real result of the hormone on the soft tissues and design the surgical plan with this information. However, this is not an absolute rule: in Spain there is no legal requirement to have started hormone treatment in order to have access to FFS. Some patients undergo surgery before starting hormone treatment, and this is a decision that must be made individually with the medical team.
FFS planning in the clinic of Dr. Richard Fakin
The Dr. Richard Fakin is a Swiss-Italian plastic surgeon with practices in Madrid and Zurich, specialising in plastic, reconstructive and aesthetic surgery with a strong background in gender affirming procedures. In his approach to FFS, preoperative planning is not a formality: it is the most important part of the process.
In the initial consultation, Dr. Fakin analyses the facial anatomy in detail, area by area, and clearly explains which procedures make sense for each case, what the expected impact of each would be, and in what order it would make sense to approach them. The goal is not to propose as many interventions as possible, but to design the most efficient plan to achieve a harmonious, natural result that is consistent with each patient's identity.
As a boutique clinic, the team devotes the necessary time to each case. This means unhurried consultations, detailed answers to all questions and support that does not end with the post-operative discharge but includes follow-up until the result is fully consolidated.
If you want to know how other patients who have been through the clinic have experienced this process, you can read about their real experiences in the Dr. Richard Fakin's testimonial page. Seeing real cases helps to gauge what to expect and to come to the consultation with a more concrete idea of what you are looking for.
What to expect during FFS recovery
Recovery from facial feminisation surgery varies considerably depending on the number and type of procedures performed. Generally speaking, swelling and bruising are the most obvious manifestations of the first few weeks and may be more intense than anticipated, especially when several procedures have been combined in the same session.
During the first few days it is common to feel tension, moderate discomfort and reduced mobility in certain areas of the face. Most patients can return to sedentary activities after 10 to 14 days, although in jobs with high social exposure it may be preferable to wait a little longer until the swelling is less visible.
The final result of FFS is not immediate. The swelling gradually decreases over weeks and months, and the scars, which in facial feminisation procedures are usually very well integrated into the hairline, the inside of the mouth or the natural folds of the skin, also evolve over time. The final result is usually assessed between six months and a year after the procedure, when all the tissues have finished adapting.
Frequently asked questions about facial feminisation surgery
Does the FFS change the face radically or are the changes subtle?
Can I have just a few procedures and add others later?
How long should I wait between one phase and the next if I do FFS in stages?
Are the scars of FFS visible?
Does the FFS have a permanent effect or does it need maintenance?
Making the informed decision with the right surgeon
Facial feminisation surgery is a process that begins long before the operating theatre. The phase of information, of reflection on which areas generate the most discomfort for you and what result you are looking for, is an essential part of the process. Arriving at the first consultation with these ideas, even in draft form, makes the planning process much more productive and the final result more in line with what you are really looking for.
Each face is unique, and a good FFS does not apply a standard protocol: it designs a specific plan for each anatomy and each goal. This is why the choice of surgeon matters so much. Not only for their technical expertise, but for their ability to listen, to analyse in detail and to explain honestly what is possible, what makes sense and what does not.
Dr. Richard Fakin's team, with offices in Madrid and Zurich, is available to accompany you from that first conversation. The first consultation is the best place to start making the plan. Make an appointment through our contact form and we advise you at all times.





































